Clinical Case Study
Patient: Female, 14 years, 105 lbs Complaints Redness, pain and




Patient: Female, 14 years, 105 lbs Complaints Redness, pain and

We normally post articles about specific pathologies or cases of

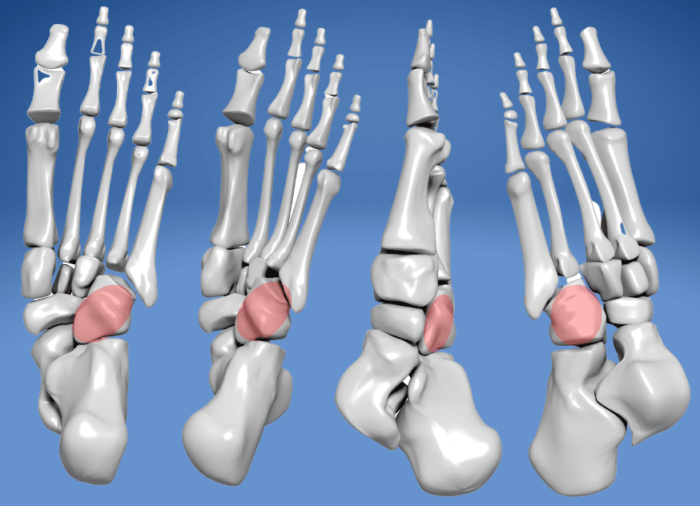
The plantar fascia is a band of connective tissue running