Case of the Season
Patient Female, age 34, 126 lbs. History and Chief Complaint

Sixu Lang, DCh, Brandon Maggen, PhD
Müller-Weiss disease is a rare condition of osteonecrosis of the lateral navicular with dorsal midfoot pain. The predominant treatment discussed in the literature is surgery. This report focuses on a single case using conservative treatment, including pain medication, ethylene vinyl acetate custom orthotics, motion control shoes, physiotherapy for strengthening intrinsic foot muscles, and weight management. The primary complaint from the patient was midfoot pain limiting activities of daily living. After application of conservative treatment modalities and 10 months of follow-up, bilateral midfoot pain decreased from 9/10 to 2/10. To the authors’ knowledge, this is the first case report of successful conservative treatment of bilateral Müller-Weiss disease in a patient with multiple comorbidities using pain medication, ethylene vinyl acetate custom orthotics, motion control shoes, physiotherapy, and weight management.
Müller-Weiss disease (MWD) is a rare condition of spontaneous osteonecrosis, lateral collapse, and fragmentation of the navicular bone with dorsal mid-foot pain that was first reported by Walther Müller and Konrad Weiss a century ago. As of 2016, only 277 cases of MWD had been reported in published articles. Müller-Weiss disease predominantly occurs in women over the age of 40 years and affects the feet bilaterally.
The pathogenesis of MWD is unclear. The cause may be a combination of abnormal biomechanical factors, decreased blood flow to the navicular, and delayed ossification of the navicular.
Typical clinical findings of MWD include insidious, long-standing dorsomedial midfoot pain, swelling, and tenderness without history of trauma. Lateral collapse of the navicular along with lateral talar head displacement pushes the rearfoot to the varus position. Wang et al. reported that six patients with MWD accompanied by medial longitudinal arch drops. Although the calcaneus remains in varus, the medial longitudinal arch drops. This paradoxical pes planus varus deformity is the hallmark of advanced MWD.
The main diagnostic investigation used in MWD is weightbearing foot radiographs with anteroposterior and lateral views. Comma-shaped deformity and fragmentation of the navicular bone are the characteristics of MWD. The rearfoot shows talar head sub-luxation, resulting in hindfoot varus and loss of the cyma line, large sinus tarsi, and retroposition of the fibula as the tibia externally rotates. The midfoot shows comma-shaped deformity and sclerosis of the navicular due to lateral collapse, talonavicular-cunei-form neoarticulation, and osteoarthrosis of the talonavicular and naviculocuneiform joints. The forefoot shows parallel metatarsal orientation and hypertrophic changes of the second metatarsal due to shift of the loading force from the first ray to the second ray.
Treatments for MWD include conservative and surgical approaches. Kitaura et al reported that prior to 1990 the majority of cases of MWD were treated conservatively and after 1990 surgical treatment was implemented when conservative therapy failed to alleviate pain. Left untreated, the disease can lead to advanced midtarsal osteoarthritis and subsequent permanent disability.
The predominant treatment discussed in the literature is surgery. Operative techniques include percutaneous drilling ecompression, talonavicular arthrodesis, talonavicular joint arthrodesis and calcaneus osteotomy,talonavicular-cuneiform arthrodesis, and triple arthrodesis (subtalar and midtarsal joints) according to the severity, surgeon’s preference, or both. Lee et al. reported midfoot and hindfoot arthrodesis with strut allograft. Tan et al. reported one case of allograft for tarsal reconstruction. Dwyer calcaneal osteotomy combined with lateral displacement may be used as an alternative to arthrodesis. Finally, vascularized bone graft has also been used.
Conservative therapy should be the initial approach. This includes custom orthotics and support footwear, nonsteroidal anti-inflammatory drugs (NSAIDs), weight management, modification of activities, and physiotherapy. Some therapeutic interventions have also included ankle-foot orthoses and cast immobilization.
We found only two published English reports of conservative therapy. Volpe et al. reported two cases of unilateral MWD that were treated using magnetotherapy, bisphosphonate injection, and custom orthotics. These two patients returned to normal life after treatment for 80 days and 4 months, respectively. Harnroongroj et al. retrospectively reviewed 68 patients with MWD who received full length, semirigid insoles and NSAIDs for at least 3 months. A total of 29 patients were deemed to have failed treatment because of persistent pain and needed surgery. The remaining 39 patients were successful and able to continue conservative treatment. There were no details regarding custom orthotics in these two reports (eg, casting method, orthotic material, and modifications).
We report one case of successful conservative treatment. We discuss the custom orthotic casting method, orthotic material, modification, and motion control shoes, which help orthotics function well. We also discuss intrinsic foot muscle strengthening and weight management as part of a holistic treatment plan.
A 74-year-old female presented with bilateral ankle pain (2/10) for approximately 1 year and bilateral dorsal midfoot pain (9/10) for 4 months. Pain was measured using the visual analog scale and the numeric pain rating scale. The pain was elicited during weightbearing activities including standing and walking. She denied any trauma history. The patient used acetaminophen/codeine 300/30 mg as needed to relieve pain. The patient also had subjective complaints of experiencing cold feet, which she reported occasionally turned blue. The patient denied using
tobacco, cannabis, or vaping products.
Medical history included osteoarthritis, which resulted in a hand deformity as well as pain in the lower back, bilateral hips, and knees. She also suffered from varicose veins, deep vein thrombosis, and a pulmonary embolism in 2008. She had heredi-
tary thrombophilia in the form of prothrombin gene mutation. The patient was advised by her hematologist to stay on long-term anticoagulant therapy. Her
current anticoagulant medication was rivaroxaban (20 mg daily). Therefore, she could not take NSAIDs and had to use acetaminophen/codeine 300/30 mg
for foot pain. The patient had essential benign hypertension, for which she had been prescribed perindopril (8 mg daily), as well as hypercholestero-
lemia, for which she had been prescribed rosuvastatin (10 mg daily). Her medical history further included a diagnosis of gastroesophageal reflux disease, for which she was prescribed rabeprazole sodium (20 mg daily). Other comorbidities included hypothyroidism, for which she took levothyroxine until 2015. The patient also had type 2 diabetes and used metformin until 2018. At the time of treatment,
her hemoglobin A1c levels were under control and she required no medication. She had a history of an incidental pituitary gonadotroph adenoma found in 2009, for which she underwent endoscopic transsphenoidal tumor removal in 2014. Most recently, she had an ascending colon polyp removed by cold snare in 2018.
The patient was 1.57 m in height and had a body weight and body mass index of 72.5 kg and 29.3 kg/m2, respectively. The patient stated that she had gained
12 kg since 2009. Bilateral pedal pulses, taken via handheld Doppler, were intact and biphasic. Bilateral toes showed redness. Her capillary refill time was
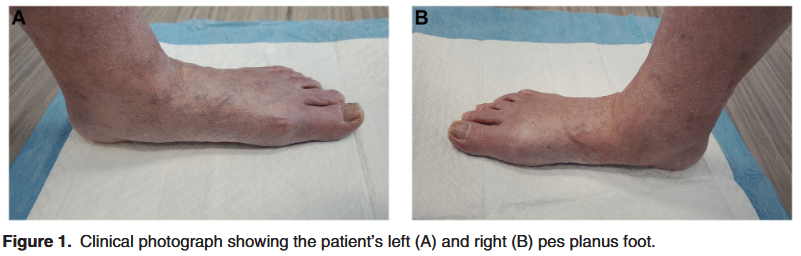
without abnormality and her bilateral foot monofilament test was intact. She had bilateral pes planus (Fig. 1), hallux limitus, and tinea pedis.
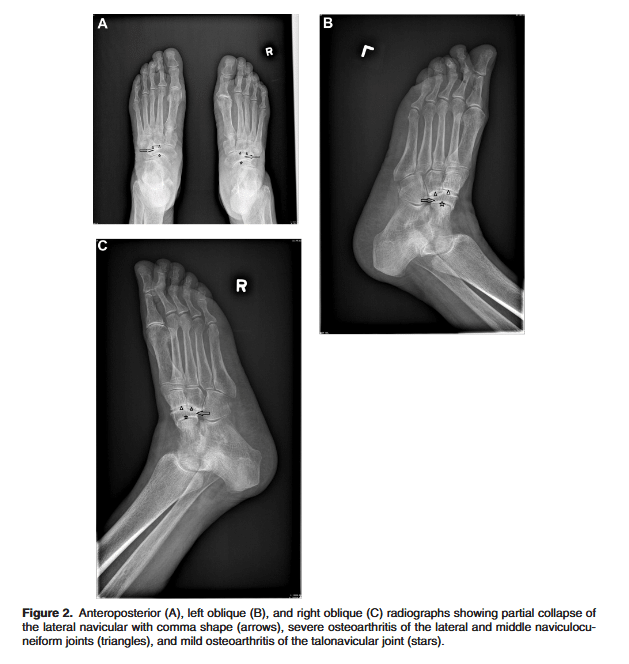
Bilateral foot radiographs were completed on November 11, 2021. Results demonstrated that the bilateral navicular bone had a partial collapse laterally, suggesting osteonecrosis, with associated severe osteoarthritis at the lateral and middle naviculocuneiform joints. There was mild osteoarthritis at the bilat-
eral talonavicular joint and no evidence of bilateral talar head subluxation. There was also osteoarthritis at the bilateral first metatarsophalangeal joint and left
second metatarsophalangeal joint. Findings suggested bilateral navicular bone osteonecrosis with secondary severe osteoarthritis at the lateral and middle naviculocuneiform joints (MWD) (Fig. 2).
The patient was hesitant to undergo any surgical interventions because of her age and comorbidities. As such, a conservative approach was taken. Her
family physician referred her to an orthopedic surgeon who agreed to the conservative treatment plan as well. Part of this approach consisted of education regarding weight loss and the effect this would have on decreasing the stress on her feet. The patient was further advised on physiotherapy exercises to
strengthen the intrinsic foot muscles. These exercises included toe lifting, toe curling, foot doming, and big toe stretching.
The patient was prescribed custom orthotics. The orthotics were cast via a nonweightbearing casting method using a three-dimensional scan with subtalar joint neutral. The orthotics were made from a 35-durometer ethylene vinyl acetate
(EVA) shell with neutral extrinsic rearfoot varus post, 14-mm heel cup, 1/8-inch microcell top cover, vinyl bottom, and bilateral Morton’s extension. Two pairs of custom orthotics were dispensed for separate indoor and outdoor use. The patient was then advised to purchase indoor and outdoor motion control shoes with a hard heel counter, hard outsole, increased torsion, and rocker forefoot to use with the orthotics.
The patient received monthly follow-up for 10 months. She lost 5 kg of body weight and stated that her bilateral dorsal midfoot pain had decreased from 9/10 to 2/10 and she had no ankle pain. She also reported that she had discontinued the use of
any pain medications and was able to return to activities of daily living.
The subject in this case study is a 74-year-old woman who experienced bilateral ankle and dorsal midfoot pain. Another cause of spontaneous osteochondrosis
of the navicular is Köhler’s disease. However, as Köhler’s disease occurs primarily in children, with unilateral presentation, and is self-limiting, it was ruled out as the cause of the patient’s condition.
The patient in this case study has a history of type 2 diabetes mellitus, body mass index of 29.3 kg/m2, and pes planus. All of these have been found to be risk factors for MWD. It is unknown whether her history of pituitary gonadotroph ade-
noma and hormone disorder is related to MWD.
She presented with pes planus deformity on weightbearing. Her resting calcaneal stance position was neutral on the left and valgus on the right. The patient did not demonstrate the hallmark of paradoxical pes planus varus, which is pes planus
with heel varus. Harnroongroj et al. found that midfoot abduction (anteroposterior Meary’s angle .13˚) and talonavicular arthritis seen on radiographs are factors contributing to the failure of conservative therapy in MWD and should be taken into consideration when determining clinical severity. In this case study, the patient
presented with talonavicular osteoarthritis on radiographs; however, she had success with conservative therapy.
Hetsroni et al. found increased plantar pressures in the midfoot as well as reduction in toe pressures in MWD patients. Custom orthotics with medial arch
support and hard platform shoes should be considered to offload midfoot pressure. The patient in this case study received orthotics with 35-durometer EVA
custom orthotics as well as motion control shoes with a hard heel counter, hard outsole, hard torsion, and rocker forefoot. The combination of custom orthotics and motion control shoes adequately supported the medial arch; limited midfoot joint motion; and facilitated heel rocker, ankle rocker, and forefoot rocker of gait. Right heel valgus changed to neutral with orthotics.
Monteagudo and Maceira suggested rigid custom orthotics with medial arch support for the sagging navicular bone and lateral heel wedge for antisupina-
tion of the varus heel. Volpe et al. did not mention the rigidity and material of the orthotics in their report. Harnroongroj et al. reported a semirigid shell but did not mention orthotic material. We used 35-durometer EVA orthotics that were not rigid. To our knowledge, this is the first case report using 35-durometer EVA custom orthotics for treatment of MWD. A lateral heel wedge was not added because
this patient did not have severe heel varus. Bilateral ankle-foot orthoses and cast immobilization were not considered for this patient because of poor compliance, the limitations this would have placed on her mobility, and increased fall risk.
Compared with the conservative treatment reported by Volpe et al. and Harnroongroj et al, we have reported more detail regarding the orthotics, such as the orthotics material, three-dimensional scan cast with subtalar joint neutral and neutral extrinsic rearfoot varus post. We addressed the importance of indoor shoes and orthotics. The patient spent most of the time indoors because of bilateral hip and knee osteoarthritis pain as well as MWD foot pain. We dispensed two pairs of orthotics and fit the orthotics in two pairs of motion control shoes for separate indoor and outdoor use. Furthermore, we used a holistic approach, including pain medication, orthotics, shoes, physiotherapy, and weight management. She also had good family and social support.
Activity modification focused on avoiding midfoot strain and decreasing the force on the navicular bone. This patient was advised on strengthening the intrinsic foot muscles to enhance the alignment of the foot and support the medial arch. Limited
weightbearing activity and weight management also helped decrease the load on the foot.
Surgical treatment should be considered only if there is failure to alleviate pain after 2 to 6 months of nonsurgical therapy. The indication for surgery is an increase in the severity of symptoms rather than the severity of deformities. After 10 months of follow-up, the patient’s bilateral dorsal midfoot pain had decreased from 9/10 to 2/10; hence, no surgical intervention was needed.
We report one case of successful conservative treatment of MWD in a patient with bilateral midfoot pain and multiple comorbidities. The finding of this case report is that MWD can be treated effectively using a holistic conservative approach, including pain medication, EVA custom orthotics, motion control shoes,
physiotherapy, and weight management.
Patient Female, age 34, 126 lbs. History and Chief Complaint

The concept of patient centered care may sound pretty basic,

Communicating the Etiology of Diabetic Foot Ulcers to Patients Gustav
| Cookie | Duration | Description |
|---|---|---|
| cookielawinfo-checkbox-analytics | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics". |
| cookielawinfo-checkbox-functional | 11 months | The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional". |
| cookielawinfo-checkbox-necessary | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary". |
| cookielawinfo-checkbox-others | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other. |
| cookielawinfo-checkbox-performance | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance". |
| viewed_cookie_policy | 11 months | The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data. |