Hypermobility & Flatfoot
Hypermobility and Flatfoot- Looking through a connective-tissue lens Steven Gillingham,

Patients with a cavus or high-arched foot frequently experience foot pain, which can lead to significant limitation in function. Custom foot or- thoses are widely prescribed to treat cavus foot pain. However, no clear guidelines for their construction exist, and there is limited evidence of their efficacy. In a randomized, single-blind, sham-controlled trial, the effect of custom foot orthoses on foot pain, function, quality of
life, and plantar pressure loading in people with a cavus foot type was
investigated. One hundred fifty-four participants with chronic musculoskeletal foot pain and bilateral cavus feet were randomly assigned to a treatment group receiving custom foot orthoses (n = 75) or to a control group receiving simple sham insoles (n = 79). At 3 months, 99% of the participants provided follow-up data using the Foot Health Status Questionnaire. Foot pain scores improved more with custom foot orthoses than with the control (difference, 8.3 points; 95% confidence interval [CI], 1.2 to 15.3 points; P = .022). Function scores also improved more with custom foot orthoses than with the control (difference, 9.5 points; 95% CI, 2.9 to 16.1 points;
P = .005). Quality-of-life data favored custom foot orthoses, although differences reached statistical significance only for physical functioning (difference, 7.0 points; 95% CI, 1.9 to 12.1 points; P = .008). Plantar pressure improved considerably more with custom foot orthoses than with the control for all regions of the foot (difference, –3.0 N . s/cm 2 ; 95% CI, –3.7 to –2.4 N . s/cm 2 ;P < .001). In conclusion, custom foot orthoses are more effective than a control for the treatment of cavus foot pain and its associated limitation in function. (J Am Podiatr Med Assoc 96(3): 205-211, 2006).
The cavus foot is characterized by an excessively high medial longitudinal arch, and it is typically re-ferred to as a high-arched or supinated foot type. The foot type may be more precisely described as a multiplanar foot deformity that usually features a varus rearfoot, a plantarflexed first metatarsal, and clawing of the digits (Fig. 1). Population-based studies suggest that the prevalence of the cavus foot is approximately 10%, and its cause is primarily idiopathic or neurogenic in nature. It is estimated that 60% of people with cavus feet experience foot pain, such as metatarsalgia, sesamoiditis, or plantar heel pain. Conditions such as these are thought to be associated with abnormal pressure loading on the plantar surface of the foot.
For at least 30 years, foot orthoses have been recommended for cavus-related foot pain because they can improve pressure distribution. In particular, foot orthoses customized to an individual have been shown to reduce and redistribute plantar foot pressure, and they are increasingly prescribed by podiatric physicians, orthopedic surgeons, and rehabilitation specialists for patients with chronic cavus foot pain. Despite these anecdotal reports in favor of custom foot orthoses, there are no clear guidelines for their construction, and there is limited evidence
of their efficacy for the painful cavus foot. To build the evidence base for orthotic therapy, we tested the effect of custom foot orthoses on foot pain, function, quality of life, and plantar pressure in people with a cavus foot type. The research design
was a prospective, randomized, single-blind, shamcontrolled trial.
A community sample of participants was recruited in Sydney, Australia, by referral from health-care providers and advertisements in the local media. Eligible participants were men and women 18 years or older who had musculoskeletal foot pain for more than 1 month and bilateral cavus feet of any etiology. The criterion for the cavus foot type was established using the Foot Posture Index, which is a diagnostic clinical tool that quantifies weightbearing foot posture and has demonstrated acceptable reliability and validity in the literature. A cavus foot was defined by a Foot Posture Index score of –2 or less, which is 2 SD below the reported normal mean of +5. Study exclusion criteria were pregnancy, recent foot trauma, current use of ankle-foot orthoses, and lack of willingness to return for follow-up. The study was approved by the Human Ethics Committee of the Uni-
versity of Sydney.
On enrollment, participants provided written consent and were randomly assigned to one of two intervention groups. Participants were informed that they would be given an orthotic device that may be different from their past experience. Members of the treatment group were fitted with a pair of custom foot orthoses molded from neutral-suspension plaster casts of the feet by an experienced podiatric physician
(J.B.) (Fig. 2). The casts were scanned using a three-dimensional laser scanner, and the orthoses were fabricated from 3-mm polypropylene using a computer-
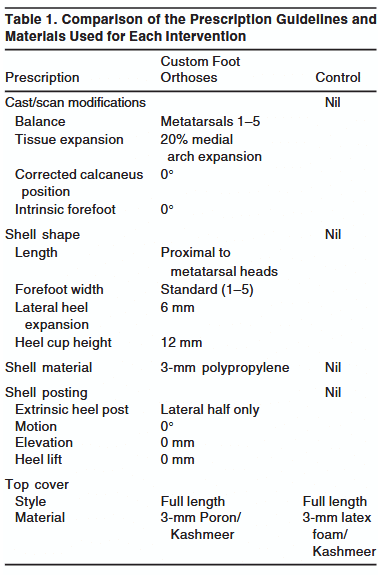
aided design–computer-aided manufacturing milling machine to a standardized prescription that had been previously developed and pilot tested. The orthoses were covered with full-length 3-mm Poron Medical urethane (Rogers Corp, Woodstock, Connecticut), which is a commonly used and effective material for
absorbing shock and reducing pressure. The exact prescription guidelines for the custom foot orthoses are shown in Table 1. The key feature of the device is the contoured flexible shell molded to the exact morphological features of the patient’s foot. With the addition of a full-length cushioned top cover, the orthotic device aims to reduce and redistribute abnormal plantar pressures.

For the control group, casts were made of both feet using the same technique as for the treatment group. However, the casts were not used to fabricate the intervention. Instead, members of the control group were given sham insoles made from flat, non-supportive, 3-mm latex foam, a material shown to be least effective at reducing pressure (Fig. 2). Both interventions were purchased from an independent supplier to avoid conflict of interest (Virtual Orthotics, Sydney, Australia). The cost was US$87 for the custom foot orthoses and US$3 for the sham insoles. Written instructions for a progressive wearing schedule and footwear advice were provided. Participants with their own orthoses, insoles, shoe inserts, and so on did not use them at any time during the study. Routine treatment, such as medication, physical therapy, and massage, were continued as usual.
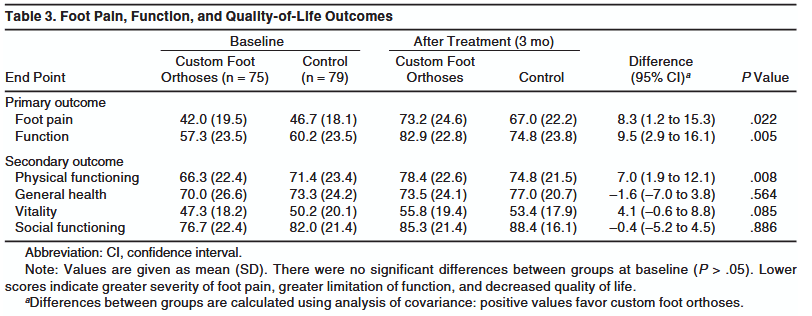
Two planned primary outcome measures, foot pain and function, were evaluated using the Foot Health Status Questionnaire at baseline and after 3 months: 0
points indicates the worst score and 100 points indicates the best score. The Foot Health Status Questionnaire was selected because it is an accurate, valid, and reliable means of measuring patient-based, foot health–specific quality of life before and after treatment.Secondary outcomes, selected before the study, were general health–related, quality-of-life measures based on four domains of the 36-Item Short-Form Health Survey: physical functioning, general health, vitality, and social functioning. These outcomes were measured at baseline and after 3 months and are included in the Foot Health Status Questionnaire.
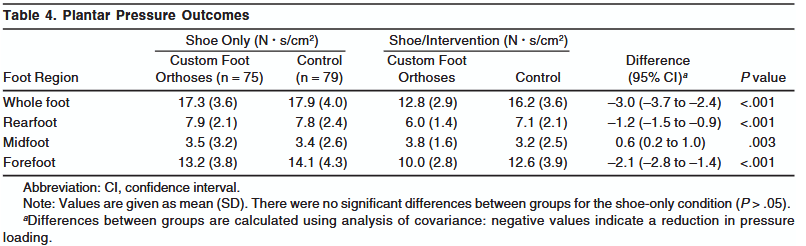
To understand the mechanism of action underlying orthotic therapy for the painful cavus foot, plantar pressure was recorded using the Pedar-mobile in-shoe system (Novel GmbH, Munich, Germany), which is an accurate, reliable, and valid measure of in-shoe pressure. Plantar pressure was measured before and after the intervention at baseline wearing a standardized shoe (Dunlop Volley; Pacific Dunlop Ltd, Melbourne, Australia) (size range, 5–12) and sock (Brooks; Texas Peak Pty Ltd, Tullamarine, Australia). After a familiarization period, data were collected at 50 Hz for approximately 40 steps on a 10-m walkway. To prevent a disturbance in gait pattern and to ensure a natural gait, cadence and walking speed were moni-
tored but not controlled. Pressure data were processed by a research assistant not involved in participant contact. Nine straight line walking steps from a random foot of each participant were selected in the Novel software (Novel GmbH). The foot was then divided into three anatomically and clinically relevant regions (rearfoot, midfoot, and forefoot) as previously reported. For each region of the foot, the pressure–time integral (N . s/cm2) was analyzed. The pressure–time integral is calculated by summing the peak pressure values that occurred in each frame of foot contact, and multiplying this by the frame interval (ie, the time for one frame). The pressure–time integral provides an understanding of the plantar pressure load distribution applied over time, and previous results suggest that it is a better indica-
tor of cavus pressure loading characteristics than either peak pressure or contact time individually.
The required sample size was estimated a priori assuming a power of 80% and an α level of .05.24 Based on historical data, sample size was calculated to detect a clinically important difference between groups of 10 (SD = 20) points in Foot Health Status Questionnaire scores,18 giving a required minimum sample
size of 67 participants in each group, with loss to follow-up of 5%.
Participants with painful cavus feet were randomly allocated to receive either custom foot orthoses or the control after their first appointment. The randomization code was developed off-site using computer-generated permuted block lengths of 4, 6, or 8 and stratified for cavus etiology (neurogenic or idio-
pathic/other). The investigator who recruited participants and potential participants was blinded to the randomization process through telephone allocation by a third party not involved in the study.
Participants were blinded to treatment allocation for the duration of the study. To encourage blinding, all of the participants in both groups had plaster casts
made of their feet at the first appointment and were advised that they would receive an intervention based on the cast parameters, although casts were used
only to fabricate the custom foot orthoses. Furthermore, extra care was taken to design an appealing, realistic, and convincing control (Fig. 2). Blinding of the investigator was not appropriate because of the potential need for ongoing contact with the participants concerning adverse effects. However, to minimize assessor bias, primary outcome measures were self-reported, and the investigator was blinded to all data entry and processing by a research assistant not involved in participant contact.
All statistical analyses were performed according to a preestablished plan (SPSS version 12.0.1; SPSS Science, Chicago, Illinois). Treatment effect was as-
sessed on an intention-to-treat basis by mean pain and function scores at 3 months using a linear regression approach to analysis of covariance (ANCOVA) to
adjust for any baseline differences between groups, with baseline pain and function scores as respective covariates, specified a priori.25 General health–relat-
ed, quality-of-life, and pressure data were also analyzed using ANCOVA, with baseline quality-of-life and shoe-only pressure data as respective covariates. Precision of treatment effect was based on the 95% confidence interval (CI) and P < .05.26
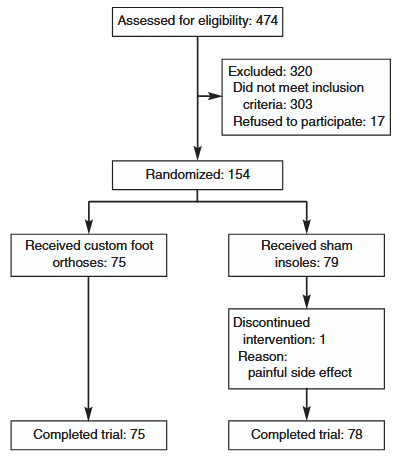
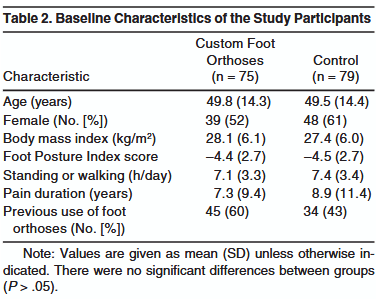
Of 474 adults screened for inclusion between December 9, 2003, and January 24, 2005, 154 (32.5%) enrolled in the trial, with 75 randomly allocated to custom foot orthoses and 79 to the control (Fig. 3). The physical characteristics of the participants were similar between groups (Table 2), and there were no differences in foot pain or function scores at baseline (P > .05) (Table 3). Cavus severity ranged from mild (Foot Posture Index score of –2) to severe (Foot Posture Index score of –12), and etiology was classified according to Statler and Tullis8 as congenital (130 patients had idiopathic and 1 had residual clubfoot), neuromuscular (16 had Charcot-Marie-Tooth disease, 4 had poliomyelitis, and 1 had polyneuropathy), or
traumatic (2 had osseous malunion). Foot pain was bilateral in 68% of the cases, and common diagnoses included metatarsalgia, plantar heel pain, and mid-
foot osteoarthritis. Overall, 153 participants (99%) were followed up at 3 months, and compliance was high, with 80% of the treatment group and 79% of the control group reporting that they wore their intervention for most of their shoe-wearing time.
In the primary analysis, mean (SD) foot pain improved 31.2 (25.8) points with custom foot orthoses and 20.3 (22.7) points with the control (ANCOVA-adjusted difference, 8.3 points; 95% CI, 1.2 to 15.3 points; P = .022). Mean (SD) function improved 25.6 (27.2) points with custom foot orthoses and 14.6 (20.6) points with the control (adjusted difference, 9.5 points; 95% CI, 2.9 to 16.1 points; P = .005). In the secondary analysis, quality-of-life data generally favored the custom foot orthoses, although differences reached significance only for physical functioning
(adjusted difference, 7.0 points; 95% CI, 1.9 to 12.1 points; P = .008) (Table 3).
In the explanatory analyses, plantar pressure loading was reduced more with custom foot orthoses than the control for the whole foot (adjusted difference,
–3.0 N . s/cm 2 ; 95% CI, –3.7 to –2.4 N . s/cm 2 ; P < .001), rearfoot (adjusted difference, –1.2 N . s/cm2; 95% CI, –1.5 to –0.9 N . s/cm2; P < .001), and forefoot
(adjusted difference, –2.1 N . s/cm2; 95% CI, –2.8 to –1.4 N . s/cm2; P < .001). At the midfoot, plantar pressure increased with the custom foot orthoses and
decreased with the control (adjusted difference, +0.6 N . s/cm2; 95% CI, 0.2 to 1.0 N . s/cm2; P = .003) (Table 4). Of note, mean (SD) contact time did not
significantly differ between groups before intervention (custom foot orthoses 756 [104] ms; control 749 [96] ms; t = 0.427; P = .670) or after intervention (custom foot orthoses 724 [92] ms; control 720 [92] ms; t = 0.302; P = .763).
Fewer adverse effects were reported with custom foot orthoses than with the control (7 [9%] versus 12 [15%]). Adverse effects were minor and included additional foot pain (4 [5%] versus 12 [15%]), ankle instability (2 [3%] versus 0), and skin irritation (1 [1%] versus 0).
There was evidence of a moderate effect for custom foot orthoses on foot pain and function in participants with a cavus foot type. Foot pain scores improved by 74% with custom foot orthoses, compared with 43% with the control. Function scores improved by 45% with custom foot orthoses, compared with 24%
with the control. From experience, this difference is clinically worthwhile, although it does not reflect how many participants completely recovered to normal levels. Resolution of foot pain to normal levels, ie, greater than 85 points on the Foot Health Status Questionnaire, occurred in 20 participants with custom
foot orthoses (27%) and 12 with the control (15%).
There is an emerging evidence base from the results of several randomized controlled trials supporting the use of custom foot orthoses for a variety of
painful foot conditions. However, there is a relative paucity of scientific literature evaluating the effect of orthotic therapy for the painful cavus foot. This study is the first randomized controlled trial to investigate the effectiveness of custom foot orthoses for treatment of the painful cavus foot.
Insights into the mechanism of the custom orthotic device were provided by the pressure-loading data. Overall, the custom foot orthoses reduced plantar
pressure by 26%, compared with a 9% reduction with the control. This threefold improvement in pressure distribution with custom foot orthoses was due to
the contoured flexible shell molded to the exact morphological features of the participant’s foot and the full-length cushioned top cover. Specifically, the cus-
tom orthotic device was shown to significantly increase pressure at the midfoot and decrease pressure at the rearfoot and forefoot, supporting preliminary hypotheses that the mechanism of pain relief is by reduction and redistribution of plantar pressure loading.
A small reduction in pressure may also explain the improvement in foot pain in the control group. Although the control group received an insole made from a material with limited shock-absorbing qualities, it was not completely inert, reducing pressure loading by 9%. This is a limitation of the study. However, if the control group had been given an insole with no pressure-reducing qualities (flat plastic, thin leather, etc), there would have been a risk of increased pain with the “harder” insole. Furthermore, convincing blinded participants of the potential merit of the
harder insole would have been difficult, and noncompliance or dropouts may have resulted. Future randomized controlled trials comparing custom foot orthoses with an inert and harmless intervention are warranted.
Custom foot orthoses generally had a greater effect on health-related quality of life than the control, particularly for physical functioning and, to a lesser extent, vitality. This indicates an increase in physical activity with the use of custom foot orthoses. These findings are similar to those of Davies et al, who reported significant improvement in physical and mental health status with the use of custom foot orthoses in an at-risk patient population with diabetes. Further research in this area investigating the overall physical and psychological benefits of orthotic therapy may prove to be most interesting in the future.
The results of this study indicate that custom foot orthoses are more effective than a control for reducing cavus foot pain and associated limitation in function.
The key feature of a successful orthotic device for this patient population is a contoured flexible shell molded to the exact morphology of the foot, with a full-length cushioned top cover. Such a device has the effect of reducing and redistributing abnormal plantar pressure loading. For patients presenting to
the clinician with painful cavus feet, custom foot orthoses are an effective treatment option.
Joshua Burns, PhD, Jack Crosbie, PhD, Robert Ouvrier, MD, Adrienne Hunt, PhD
Article from Journal of the American Podiatric Medical Association
Hypermobility and Flatfoot- Looking through a connective-tissue lens Steven Gillingham,
Patient: Female, 14 years, 105 lbs Complaints Redness, pain and

We normally post articles about specific pathologies or cases of
| Cookie | Duration | Description |
|---|---|---|
| cookielawinfo-checkbox-analytics | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics". |
| cookielawinfo-checkbox-functional | 11 months | The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional". |
| cookielawinfo-checkbox-necessary | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary". |
| cookielawinfo-checkbox-others | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other. |
| cookielawinfo-checkbox-performance | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance". |
| viewed_cookie_policy | 11 months | The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data. |