
Hallux Limitus
Hallux Limitus is a condition causing inflammation and soreness

Gustav Jarl, PhD, Jaap J. van Netten, PhD, Peter A. Lazzarini, PhD
People at risk for diabetic foot ulcer (DFU) often misunderstand why foot ulcers develop and what self-care strategies may help prevent them. The etiology of DFU is complex and difficult to communicate to patients, which may hinder effective self-care. Thus, we propose a simplified model of DFU etiology and prevention to aid communication with patients. The Fragile Feet & Trivial Trauma model focuses on two broad sets of risk factors: predisposing and precipitating. Predisposing risk factors (eg, neuropathy, angiopathy, and foot deformity) are usually lifelong and result in “fragile feet.” Precipitating risk factors are usually different forms of everyday trauma (eg, mechanical, thermal, and chemical) and can be summarized as “trivial trauma.” We suggest that the clinician consider discussing this model with their patient in three steps: 1) explain how a patient’s specific predisposing risk factors result in fragile feet for the rest of life, 2) explain how specific risk factors in a patient’s environment can be the trivial trauma that triggers development of a DFU, and 3) discuss and agree on with the patient measures to reduce the fragility of the feet (eg, vascular surgery) and prevent trivial trauma (eg, wear therapeutic footwear). By this, the model supports the communication of two essential messages: that patients may have a lifelong risk of ulceration but that there are health-care interventions and self-care practices that can reduce these risks. The Fragile Feet & Trivial Trauma model is a promising tool for aiding communication of foot ulcer etiology to patients. Future studies should investigate whether using the model results in improved patient understanding and self-care and, in turn, contributes to lower ulceration rates. (J Am Podiatr Med Assoc 113(1), 2023)
Diabetic foot ulcers (DFUs) are a common and devastating complication of diabetes and are associated with infections, amputations, and reduced life expectancy. Approximately 19% to 34% of people with diabetes will develop at least one DFU during their lifetime. Although most DFUs heal, approximately
40% of patients will develop another DFU within 1 year of healing, and this figure increases to 60% within 3 years of healing. Many of those DFUs may have been prevented with regular screening and integrated foot care of people at risk for DFUs. However, most of the prevention efforts depend on patients’ engagement with self-care practices, such as wearing appropriate footwear, inspecting their feet for preulcerative lesions, and lubricating dry skin. Although several factors may contribute to low adherence to self-care activities, one potential factor is a combination of limited understanding among patients of the DFU etiology and a perceived lack of control in preventing DFUs, resulting in lack of engagement in self-care. Resolving this lack of understanding and engagement relies on patient education and good communication between patient and health-care practitioner.
The International Working Group on the Diabetic Foot strongly recommends that people at risk for foot ulceration be provided structured foot self-care education although its evidence base is weak. A recent systematic review found only seven randomized controlled trials investigating whether structured education about foot self-care can prevent DFUs. The content of the education was not described in detail in all seven of the studies, but in at least four of the studies aspects of DFU etiology were included in the education. This finding indicates that it is generally believed that DFU etiology is an important aspect of foot self-care education.
Communicating DFU etiology is challenging because the etiology is complex and includes a variety of interacting risk factors, and there is often limited time available in clinical practice to explain such a challenging etiology. Adding to this complexity, each individual risk factor may or may not play a role in the evelopment of DFU in each individual patient; for example, one study found 32 unique pathways to DFU. Explaining risk factors that are not applicable to an individual patient may
even be disengaging when a patient does not recognize these risk factors in themselves. Additional to these challenges are varying levels of health literacy and potential cognitive impairments. Together, this situation can leave many patients
misunderstanding how foot ulcers develop, resulting in little or even counterproductive self-care practices in DFU prevention. Thus, there is a need for tools to support the communication of DFU etiology to patients. We aimed to propose a simple model of DFU etiology to aid communication with patients to improve their understanding of the etiology and their engagement in self-care to
prevent DFUs.
Communicating with patients can positively or negatively affect treatment outcomes. Good communication provides opportunities to enhance an individual’s motivation for self-care while simultaneously increasing trust and understanding between patient and professional. Conversely, poor communication may negatively affect self-care and the relationship between patient and professional. Communication concerns the process of exchanging information, and both the content and the language used are important. For a patient to understand the content, it should match their cognitive capacity and their individual situation. The
language used when communicating, both verbal and written, should be based on patients’ strengths, should be bias-free and person-centered, and should align with important recommendations from expert communication bodies such as the Association of Diabetes Care & Education Specialists. Hence, to be aligned with these communication recommendations, a model for DFU etiology to aid patient communication should consider using the acronym SIC:
• Simple: The model should explain DFU etiology as simply as possible, for example by “chunking” together several risk factors and using straightforward language to label them.
• Individual: The model should support communication tailored to the individual, for example by having a general framework that can be adjusted to fit the context and specific risk factors of the individual patient.
• Clear: The model should provide clear strength-based health messages, such as what self-care activities the patients can do to reduce their risk of DFU.
However, there is currently a scarcity of models and tools to support the communication of DFU etiology to patients. This leaves clinicians having to
find ways to explain a complex and and multifactorial etiology in layman’s language.
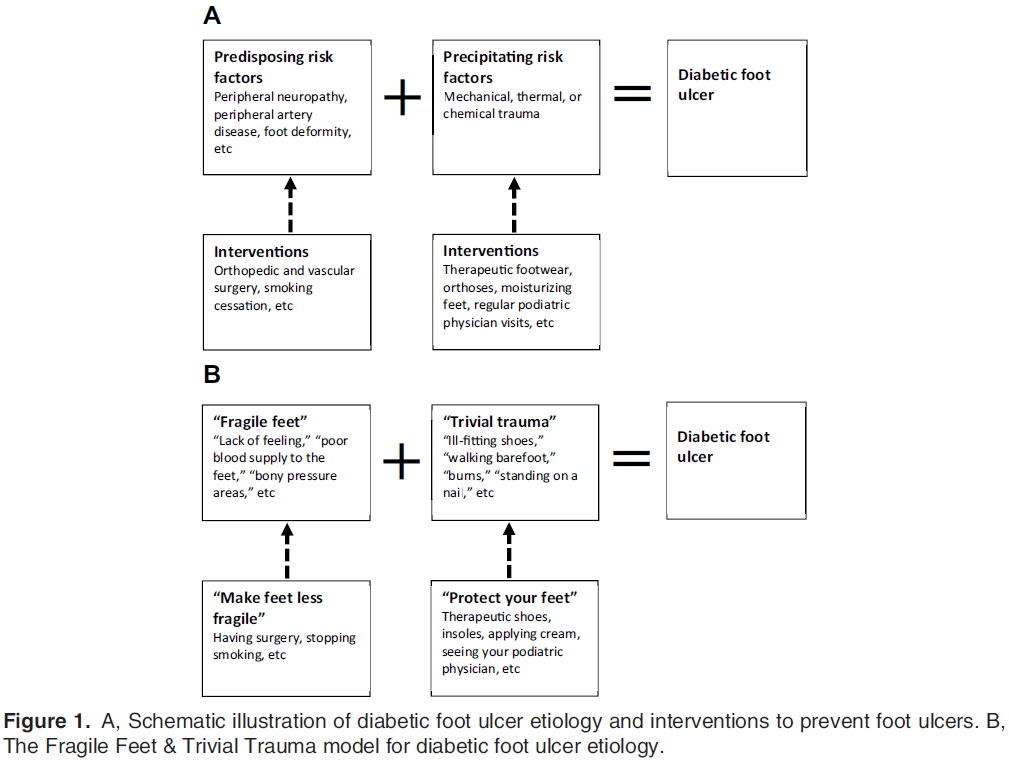
The risk factors for DFUs are well-known and can be divided into predisposing and precipitating risk factors; in combination, these often result in foot ulcers, as schematically illustrated in Fig. 1A.
One of the most important predisposing risk factors is peripheral neuropathy, which comes in three forms, all of which increase the risk of foot ulceration.
First, sensory neuropathy results in loss of protective sensation, which significantly increases the risk that patients do not experience a normal pain response to trauma. Second, motor neuropathy results in muscle weakness, gait changes, and
foot deformities, which all increase mechanical plantar pressures when standing and walking. Third, autonomic neuropathy reduces sweating and results in dry skin that is prone to crack and develop callus, which also can increase plantar pressures. The other major predisposing risk factors are peripheral artery disease (PAD), which means that little external pressure is needed to impede blood supply in the feet, and preexisting foot deformities, which means that dangerous high
mechanical plantar pressures may already be present. Although surgical interventions can sometimes improve foot deformities and PAD, the predisposing
risk factors in most cases remain for the rest of the patient’s life. No matter the patient’s specific combination of predisposing risk factors, the result is that patients have a lifelong increased risk of developing foot ulcers. In recognition of these predisposing risk factors lasting for the rest of life, we suggest communicating these risk factors using the simpler term of “fragile feet” for life.
Although patients may have an increased risk of developing ulcers, to actually go on to develop such an ulcer typically also requires a precipitating risk factor.
Precipitating risk factors are different forms of trauma: often mechanical trauma (eg, high plantar pressure), sometimes thermal trauma (eg, burns
and frostbite), and occasionally chemical trauma (eg, chemical agents to remove corns or callus). Mechanical trauma can be divided into three categories based on the mechanical forces’ magnitude, the number of loading cycles, and the duration.
First, a single occasion of high forces can disrupt the skin and cause a DFU. For example, patients may step on something sharp when walking barefoot,
drop something heavy on the foot, or bump the foot on furniture. Second, numerous loading cycles can cause local foot inflammation and subsequent
ulcers although the force may be of moderate magnitude. Such cycles typically occur on the plantar surface of the foot when walking without footwear or in footwear that does not sufficiently redistribute plantar pressures, especially in people with foot deformities. Third, prolonged pressures can cause foot ulcers even if pressures are low, especially if the person has PAD. These pressures can arise on the heels when a person is lying supine in bed or on the toes if a person wears tight-fitting footwear. For people with good protective sensation (ie, without
sensory neuropathy), prolonged pressures may cause discomfort and pain, causing them to take action to reduce the pressure, for example, by limping,
shifting position in bed, or removing their footwear. However, for people with sensory neuropathy, there is often no discomfort or pain in response to
such trauma, and hence foot ulcers may appear for rather trivial reasons. Although these precipitating risk factors are trivial and typically do not result in ulcers in those without predisposing risk factors, such as neuropathy, who can “naturally” detect and protect against these precipitating risk factors, in those with predisposing risk factors, this seemingly “trivial trauma” can be the trigger for ulcer
development.
The Fragile Feet & Trivial Trauma model for DFU etiology is based on the simplified scheme for DFU etiology (Fig. 1A) wherein the numerous potential risk factors are chunked or grouped into the overarching categories of predisposing risk factors and precipitating risk factors. Because these terms may be unfamiliar to many people, we suggest to instead use the terms fragile feet and trivial trauma,
respectively (Fig. 1B). For the same reason, everyday language should be used rather than medical jargon to describe the risk factors. For example, “poor blood supply to the feet” is preferable to “peripheral artery disease,” “lack of feeling” or “numb feet” are preferable to “sensory neuropathy,” and “bony pressure areas” is preferable to “foot deformity.” Figure 1B illustrates how the terminology for describing the DFU etiology can be simplified when communicating with patients. To keep things individual for each patient, only the predisposing and precipitating risk factors that apply to the specific patient should be communicated. A clear message to patients is that they will have an increased risk of foot ulceration for the rest of their life because of fragile feet and that it only takes a trivial trauma to
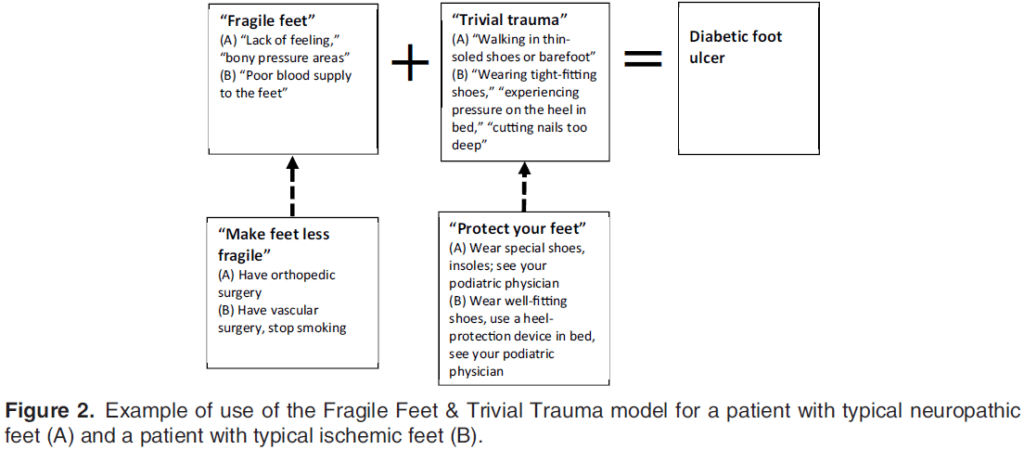
start a new foot ulcer. After the patient has understood these ideas, the clinician and patient can discuss and agree on interventions to reduce the fragility of the feet and protect the feet from trivial trauma to reduce the risk of developing DFUs. In the following two sections, two fictional but typical patient cases based on clinical encounters of one of us (G.J.) and his application of the model are used
to illustrate how the Fragile Feet & Trivial Trauma model might be used in patient education.
The etiology of DFUs is complex, and patient misunderstanding of the etiology may be one of the things that prevent effective self-care to reduce DFU risks. We proposed a simple and patient-centric model, the Fragile Feet & Trivial Trauma model, that can be integrated into the (structured) patient education that typically occurs in everyday clinical encounters. The model can be used to discuss DFU
etiology and interventions with patients in three key steps: 1) how the patient’s specific predisposing risk factors make the patient’s feet fragile, 2) how specific trivial trauma in the patient’s environment is enough to produce a DFU on the patient’s fragile feet, and 3) reaching agreement on concrete measures that the clinician and the patient can take to reduce the fragility of the patient’s feet and protect them against trivial trauma with the aim of reducing the risk of future DFUs.
The thinking behind the Fragile Feet & Trivial Trauma model is built on key recommendations from general patient-clinician communication, as outlined in the first part of the article. Although several authors have summarized DFU etiology in flowchart type diagrams in the past,these diagrams are less useful in patient education because they are typically complicated and written in medical jargon.
The Fragile Feet & Trivial Trauma model also fits well with other studies in the field of diabetes-related foot disease, where changes of terminology and communication style have been suggested to highlight and communicate
specific aspects of diabetes-related foot disease. For example, Armstrong and Mills suggested that a healed foot ulcer should be referred to as “in remission” rather than as “healed” to emphasize the high risk of repeated ulceration and the need for frequent follow-up and prompt intervention. Furthermore, Price stressed the importance of breaking down important information into small chunks to improve adherence to DFU preventive treatments. Finally, Jarl and Lundqvist suggested the concept of “latent diabetic foot disease” to emphasize that the presence of predisposing risk factors increases the risk of DFUs even during periods when foot disease is less evident. The Fragile Feet & Trivial Trauma model builds on these thoughts and adds a structure for communicating DFU etiology and interventions to patients. Future research should investigate whether use of this model results in improved understanding of DFU etiology among patients and, subsequently, in better self-care and fewer DFU outcomes.
One of us (G.J.) has used the Fragile Feet & Trivial Trauma model in clinical encounters with patients attending a multidisciplinary diabetic foot team. The author found it to be useful when discussing DFU etiology and self-care with patients, where the intuitive concepts easily fit into an informal conversation. He (G.J.) has also used the visual representation of the model (Fig. 1B) when teaching DFU etiology to students and medical professionals not specialized in diabetes-related foot disease.
However, because the model simplifies the etiology of DFUs, it does come with certain limitations. The model assumes that DFUs develop as a consequence
of a combination of predisposing and precipitating risk factors. This assumption is true for most DFUs, but there are scenarios in which a single factor, such as a trauma, edema, or a spontaneous skin crack, can cause a DFU. In those cases, the model is less useful for communicating DFU etiology. However, when the etiology involves only one factor, it can be communicated easily without using any model.
In the end, we can expect patients to be more motivated and engaged in appropriate self-care to reduce their risks of developing DFUs if we make sure that
they understand how DFUs develop and how certain self-care actions help prevent DFUs. When using the model, a nonjudgmental attitude is important. For example, the precipitating risk factors (or the trivial trauma) are part of everyday life, and it can be ssumed that all people occasionally step on something sharp or bump their foot on something hard. This is important to keep in mind when asking patients to avoid all things that can initiate a DFU. This challenge is extremely complex and requires significant daily efforts to be performed for many years. Hence, we should try to minimize any perceived shame that patients who develop new foot ulcers may feel and instead encourage them to perform self-care and to immediately contact a health-care provider when in need of help.
We proposed a simple model, the Fragile Feet & Trivial Trauma model, to aid in communication of DFU etiology and interventions to patients. Future research should investigate whether using this model results in improved patient understanding of the etiology and more appropriate self-care practices and, in turn, contributes to lower DFU rates.
Hallux Limitus is a condition causing inflammation and soreness

Patient Female, 62 years old, 165 lbs. Complaints Pain at

When considering older patients in any context it’s best to
| Cookie | Duration | Description |
|---|---|---|
| cookielawinfo-checkbox-analytics | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics". |
| cookielawinfo-checkbox-functional | 11 months | The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional". |
| cookielawinfo-checkbox-necessary | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary". |
| cookielawinfo-checkbox-others | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other. |
| cookielawinfo-checkbox-performance | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance". |
| viewed_cookie_policy | 11 months | The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data. |