
Increasing Your Orthotic Productivity
If you are interested in prescribing more orthotics, this article
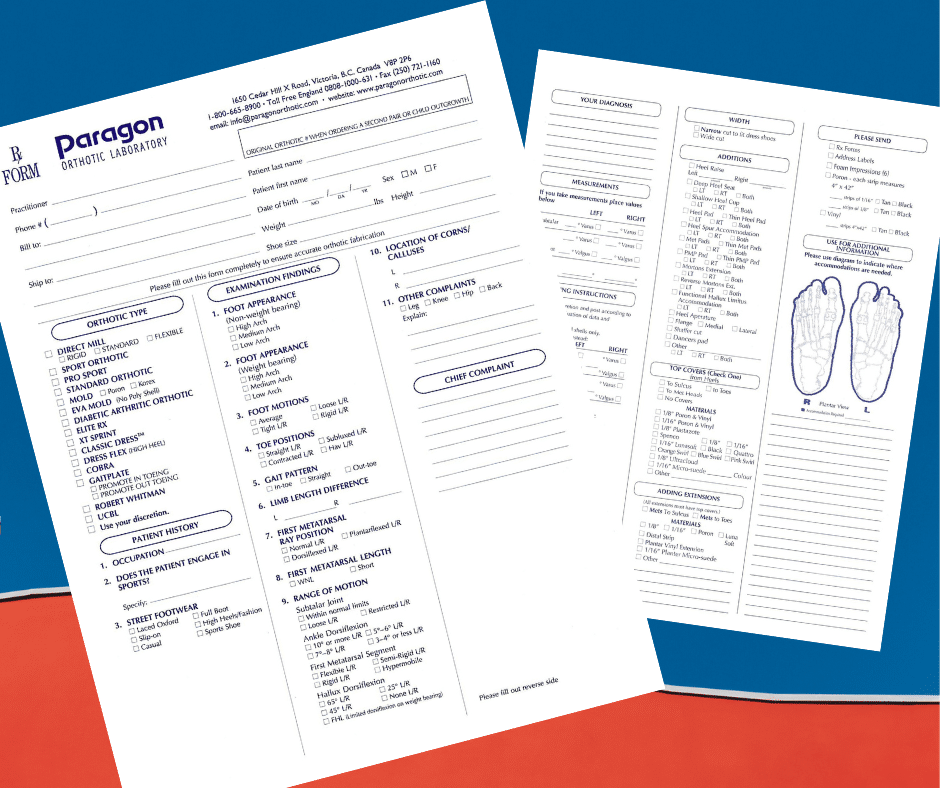
Years ago we redesigned our prescription form to not only include specifications for orthotic fabrication, but also biomechanical examination findings, patient history, and measurements. This information is handy for practitioners to have in one document in the patient’s file, but also for your orthotic manufacturers to have a complete picture of the case. From this information the type of orthosis, posting systems, additional requirements and ultimate success of your treatment will be determined.
We will briefly review these sections to enhance clarity and understanding when supplying this vital information.
** Please always include the patient’s weight and shoe size. This information is vital in fabricating the right device for your patient.
Measurements are very helpful but not always necessary for your orthotic manufacturer. To order orthotics based purely on measurements can be a serious mistake. They have to be considered along with all the other information.
As a general rule, the more information you provide to your orthotic manufacturing lab the better. Our qualified technicians are able to carefully create a custom instrument for your patient based on a variety of factors and data, including the important information provided on your prescription form.

If you are interested in prescribing more orthotics, this article
“Experience is the one thing you can’t get for nothing.”
Patient Female, age 34, 126 lbs. History and Chief Complaint
| Cookie | Duration | Description |
|---|---|---|
| cookielawinfo-checkbox-analytics | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics". |
| cookielawinfo-checkbox-functional | 11 months | The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional". |
| cookielawinfo-checkbox-necessary | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary". |
| cookielawinfo-checkbox-others | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other. |
| cookielawinfo-checkbox-performance | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance". |
| viewed_cookie_policy | 11 months | The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data. |