
Increasing Your Orthotic Productivity
If you are interested in prescribing more orthotics, this article

In a previous blog, we delved into the wondrous and complex structure and function of the foot. The two main functions of the foot are shock absorption and propulsion. In order to accomplish these tasks, our feet are made up of a variety of bones, muscles, and ligaments, all arranged in a specific mechanically efficient and successful way. The incorrect arrangement can lead to many problems with not only the foot, but all the way up the kinetic chain.
The main contributors to the function of shock absorption are the longitudinal and transverse arches of the foot. But these structures also play a role in protection and stability. Being able to accurately and purposely evaluate the correct shaping of the foot is important for all foot specialists because of the detrimental effects of deformation. In this article we will take a look at the Foot Posture Index (FPI-6) as a means to quickly and easily evaluate the feet.
The FPI-6 was developed to be useful as a diagnostic tool in a variety of ways. It can be used to determine biomechanical risk factors for certain issues, investigating the relationship between foot type and certain risk factors, identifying foot type and patient classification for therapeutic purposes, and a means of assessing differences in foot structure. As this tool is used during standing, it can be an important tool to use alongside the gait analysis and assessments already used.
While using the FPI-6, the clinician uses six separately evaluated criteria to rate the posture of the foot. The six features are rated on a scale of -2, -1, 0 (neutral), +1, +2, whereas pronation is positive and supination is negative. The more positive or negative the rating, the more severe for deformation.
The total result classifies the foot into the following categories:
The patient stands in a relaxed, comfortable, and still stance. The clinician observes the front and back of the foot and makes assessments based on the 6 criteria in the table below. Please see summary table and descriptions below.
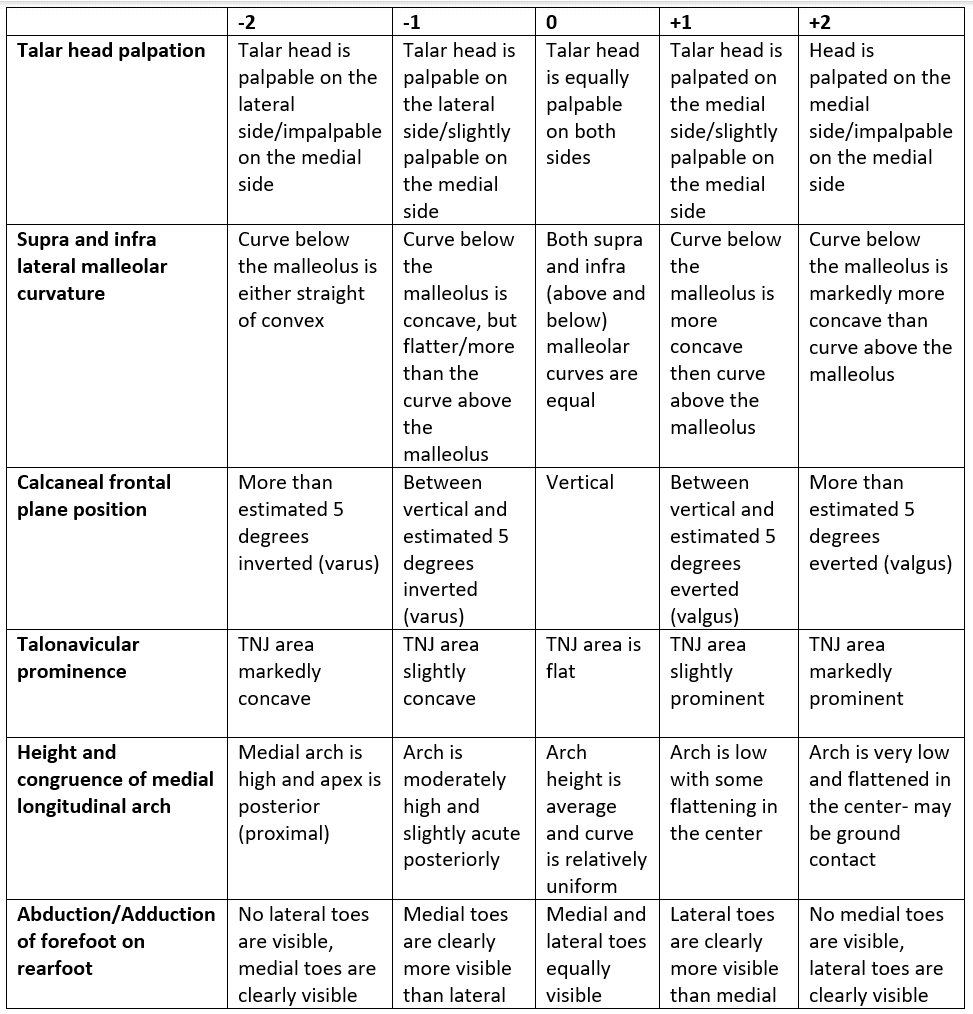
Talar head palpation- clinician palpates the medial and lateral side of the talar head.
Supra and infra lateral malleolar curvature- clinician views the malleolus from behind. In a neutral foot the curvature above and below the malleolus will look the same/be equal. In a pronated foot, the abduction of the foot causes the the curve below the malleolus becomes greater than the one above (it is more concave).
Calcaneal frontal plane position- clinician views the foot from behind in the frontal plane and estimates the degree of calcaneal inversion or eversion in relation to the longitudinal axis.
Talonavicular prominence- clinician views the bulging of the talonavicular area from behind at an angle to the medial side of the foot. In a neutral foot, the area is relatively flat. In a pronated foot, the area will be concave, whereas in a supinated foot the bulging will become more prominent (convex).
Height and congruence of medial longitudinal arch- the clinician views the arch from the medial side. In a neutral foot the curvature of the arch will be relatively uniform throughout the span of the arch. In a pronated foot, the curvature becomes flattened in the center. In a supinated foot, the apex of the arch will be more proximal.
Abduction/adduction of the forefoot on the rearfoot- the clinician views the forefoot from behind the foot. In a neutral foot, the forefoot will be visible equally on both sides. In a supinated foot, the forefoot is abducted in relation to the ankle and will be more visible on the medial side. In a pronated foot, the opposite is true, and the toes are more visible on the lateral side.

If you are interested in prescribing more orthotics, this article
“Experience is the one thing you can’t get for nothing.”
Patient Female, age 34, 126 lbs. History and Chief Complaint
| Cookie | Duration | Description |
|---|---|---|
| cookielawinfo-checkbox-analytics | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics". |
| cookielawinfo-checkbox-functional | 11 months | The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional". |
| cookielawinfo-checkbox-necessary | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary". |
| cookielawinfo-checkbox-others | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other. |
| cookielawinfo-checkbox-performance | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance". |
| viewed_cookie_policy | 11 months | The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data. |