
Increasing Your Orthotic Productivity
If you are interested in prescribing more orthotics, this article


So often we are asked to evaluate patients who have failed orthotics from another provider. This article is designed to assist you in evaluating the quality of orthotics and what you can do to facilitate better treatment results. The field can be confusing for the patient, as it is unregulated and anybody can claim to make orthotic devices.
To begin, it is important to identify the patient’s pathology and biomechanical problems. Convey your findings to the patient prior to evaluating their current orthotics. A lot of the time, their current appliance is not the proper one for their condition. Perhaps it is not a real prescription orthotic, but simply an arch support.
After you have identified the problem, explain and describe the type of orthotic they need to correct it. Then, evaluate the current device, and offer to remake it properly if it is inappropriate for their needs. If it was made correctly, the next step is to evaluate their shoes, activities, etc. The patient may choose to continue with a more invasive treatment, but it is still important to let them know the importance of properly made orthotics, so as to prevent exacerbation and/or recurrence of the problem.
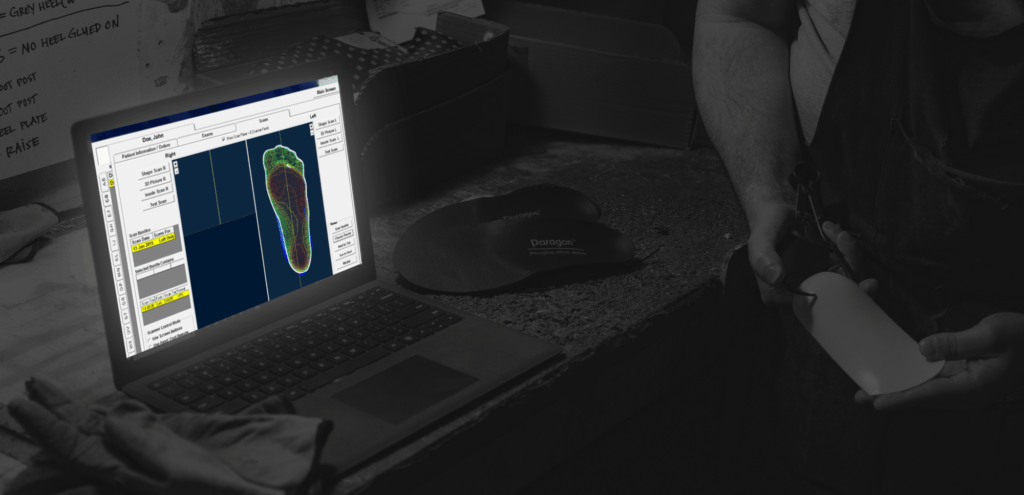
When evaluating orthotics for a specific patient, we are looking at multiple processes. Was the original cast or image was done accurately? Was the orthotic made properly from that cast or image?
The basic premise in fabricating orthotics is trying to position the patient’s foot in or near subtalar neutral position with the metatarsal joint fully pronated. This allows optimal shock absorption at contact by allowing subtalar global joint pronation, which is where the main shock of absorbed. Then, in late heel contact and through midstance, the midstarsal joint is pronating and adapting to terrain. After midstance the pronation stops and resupination of the subtalar joint begins with external tibial rotation. This is caused by rotation of the upper skeleton. There is reduced range of motion of the midtarsal joints, as they convert to a rigid lever, which allows the patient to push off from the stable support.
If any of the following criteria for proper orthotic fabrication is violated or inaccurate, you will have compromised the correction of the patient’s walking. When evaluating a patient’s orthotic, be sure to evaluate for flexibility, shape, balance, and length.

The orthotic must be strong enough to withstand the patient’s body weight, foot deformity and correction. Here we are evaluating the strength of the orthotic. If the material is too flexible, it will not be able to adequately resist abnormal motions and will be ineffective in influencing foot functions. If the material is too rigid, it will be uncomfortable and won’t allow adequate shock absorption.
The shape of the orthotic is critical to proper performance of the orthotic. To check shape, hold the patient’s foot in a subtalar neutral position with the midtarsal joint pronated. This is typically the standard casting technique position. Then, softly hold the orthotic plate up to the foot. You should see the close contour between the bottom of the foot and the top of the orthotic. In cases of forefoot imbalance, you should see a qualitative flare of the plate from the foot medially. For valgus, the opposite is the case, as you should look for flare laterally under the fourth and fifth metatarsal necks. In zero balance, you should see close contact in the entire plate to the foot. The only area of gap should be approximately 5mm medial to the first metatarsal shaft to account for soft tissue expansion, which occurs in weight bearing. If there is too much gap, it will allow over pronation as the plantar foot attempts to become plantar grade and there will be a lack of contact as the foot falls to the floor. The only danger of any inadequate gap in the medial arch may be irritation. You can heat adjust this or grind it down to allow expansion to occur.
The shape is influenced by numerous factors. The first is the shape of the original cast taken by the practitioner. If the patient’s foot was supinated at the subtalar joint, the forefoot measurement will be more varus and the patient will pronate off the orthotic. If the patient’s foot was supinated at the midtarsal joint, there will be excessive varus balance as well as a gap in the medial arch. Oversupination of the oblique axis will cause flaring of the plate from the foot medially and laterally, since the oversupination caused the original foot shape to be exaggerated in the sagittal plane. Excess pronation of the subtalar joint in casting the foot will show too much valgus balance or inadequate valgus, depending on the neutral measurements of the patient’s foot.
You can detect these different findings by determining the difference in the shape of the plantar foot as well as the frontal plane relationships of the forefoot and rearfoot and different joint positioning.
The orthotics must have the right amount of correction or tilt based upon your foot measurements. Checking orthotic posting or balance is similar to measuring the forefoot and rearfoot. With the patient in the prone position you place the subtalar joint with the midtarsal joints locked/pronated. The legs should be in or close to simulating the base of gait in relation to the long axis of the spine.
Holding the orthotic softly against the plantar surface of the foot, look at the plantar surface of the orthotic. Think of the orthotic’s plantar surface as a plane using the distal medial, distal lateral, and plantar heel contact points to define that plane. We visually compare the plane to the horizon or anticipated walking surface. The tewo places should be parallel. This shows that when the patient stands on the orthotic their subtalar midtarsal joints will be in the proper position.
It is critical to evaluate the length and width of an orthotic in order to ensure proper fit, comfort, and control. The distal end of the orthotic has to be just proximal to the metatarsal heads. The best way of measuring this is to palpate the metatarsal heads with your thumb. But a red dot where you feel the center. You can mark all of the metatarsal heads but especially the first, second, and fifth. This will give you the proper parabola of how the orthotic should have been cut. The forefoot is a hinge joint and it has to bend at that hinge. If the orthotic underrides any part of that hinge it will throw the foot off considerably.
If the orthotic is too short (shorter than 5mm from the center of the metatarsal head), it may need to be remade. This will not control the forefoot properly and can cause numerous problems. Orthotics made short can feel quite comfortable but will actually cause less correction and result in more acquired deformity.
Assessing the intrinsic quality of your orthotics is a crucial step toward ensuring your patient receive the care they deserve. It’s important to hold your manufacturing lab accountable for the products they create for you. At Paragon, we want you to get the products you ask for. Our technicians are highly skilled and experienced, and our customer service team is always here for you.
If you are interested in prescribing more orthotics, this article
“Experience is the one thing you can’t get for nothing.”
Patient Female, age 34, 126 lbs. History and Chief Complaint